
.png)

Her name was Diana. Forty-four years old, a high school principal, and — by her own description — someone who had been "sick" for three consecutive winters in a row.
Not catastrophically sick. Just chronically, relentlessly, functionally sick. Facial pressure that made her feel like she was wearing a lead mask. A headache that sat behind her eyes every afternoon. A smell she could barely detect anymore — not entirely gone, but muted, like hearing a voice through a closed door. And a fatigue that no amount of sleep seemed to touch.
She had seen three physicians over those three years. She had completed four courses of antibiotics. She had tried nasal sprays, allergy pills, steam, and a neti pot she'd bought on the recommendation of a podcast.
"I feel like my head is full," she told me. "All the time. Not congested, exactly. Just... full."
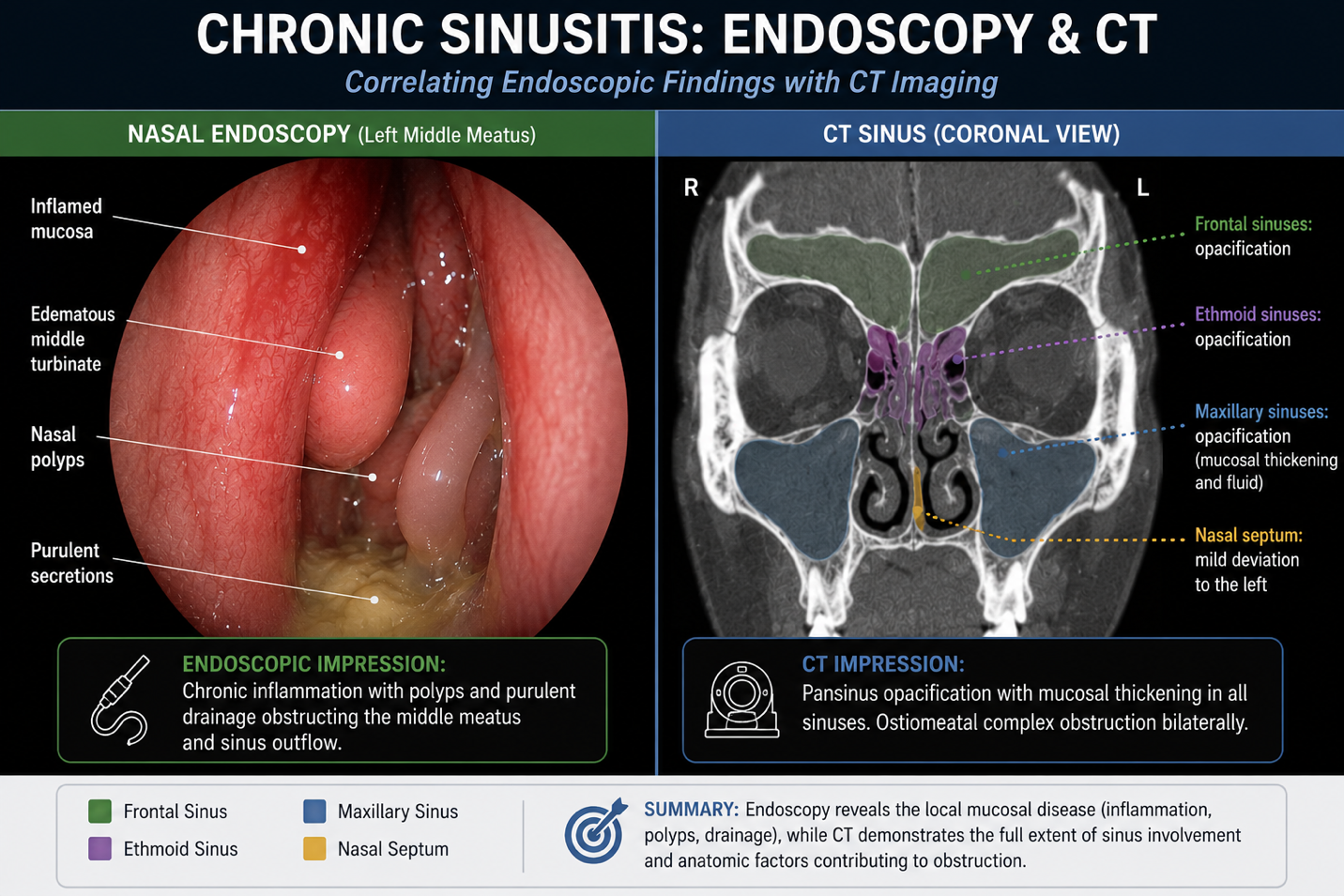
The nasal endoscopy told the story clearly: chronic sinusitis with significant mucosal thickening around the sinus drainage pathways. Her sinuses weren't infected in that moment — but they had been inflamed long enough that the outflow tracts were narrowed, the lining was swollen, and the system that was supposed to drain, ventilate, and clear itself had essentially stopped working.
Her sinuses had become a sealed chamber. And when a chamber can't drain, pressure builds — whether we're talking about a nasal sinus or a Formula 1 intake manifold.
🔧 TECH SPEC BRIEFING — The Engineering Behind the Anatomy
“The Plenum Chamber”
🔧 TECH SPEC
In a turbocharged Formula 1 engine, compressed air from the turbocharger doesn't flow directly into each cylinder. It first enters a structure called the plenum chamber — a pressurized manifold that acts as an equalizer. The plenum receives high-pressure charge air and distributes it evenly and smoothly to each cylinder's intake port. Without it, cylinders would compete for air, pressure would fluctuate wildly, and performance would be inconsistent and unpredictable.
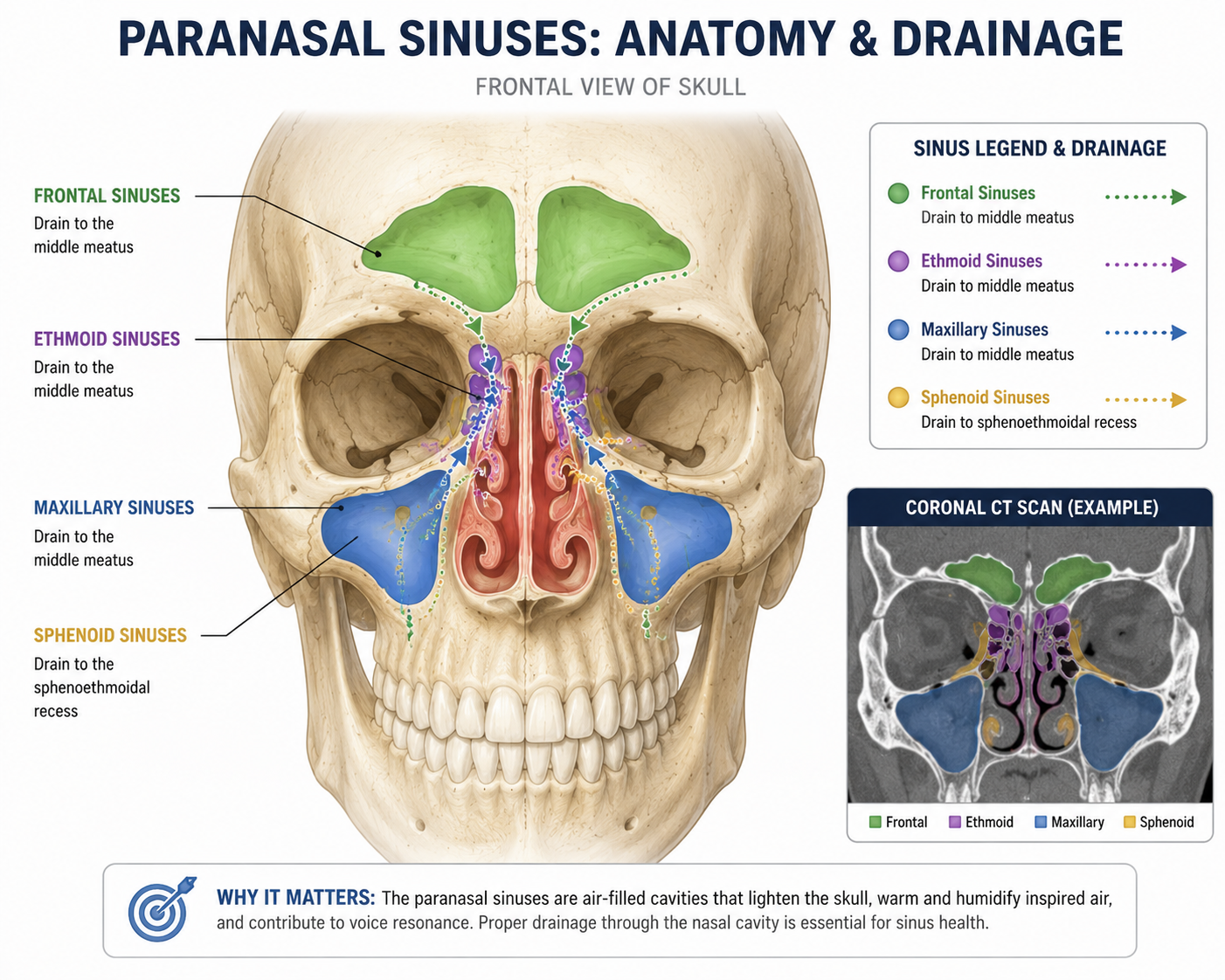
Your sinuses work on the same principle. The four paired sinus cavities — frontal, maxillary, ethmoid, and sphenoid — are not simply decorative holes in your skull. They are pressurized chambers that communicate with your nasal airway through narrow drainage openings called the ostiomeatal complex. Their job is to condition, equalize, and maintain the pressure environment of your nasal airway — and to produce a thin layer of mucus that flows continuously, trapping particles and moving them toward the throat for clearance.
When the drainage openings narrow or close — from inflammation, infection, polyps, or anatomy — the plenum chamber seals. Pressure builds. Mucus stagnates. Bacteria thrive. And the downstream performance of your entire airway degrades.
The Four Chambers: A Map of Your Pressure System
Most people think of sinusitis as a single condition affecting one vague region of the face. In reality, there are four distinct pairs of sinus cavities, each with its own location, drainage pathway, and failure signature.
- Frontal sinuses — located above your eyebrows, behind the forehead. When these are blocked, you feel a heavy pressure across your forehead, worse in the morning when you first stand up. Up to 10–15% of people never fully develop frontal sinuses at all — a normal anatomic variant.
- Maxillary sinuses — the largest sinuses, located behind your cheekbones on either side of the nose. Maxillary sinusitis often mimics a toothache along the upper jaw. This is one of the most commonly confused diagnoses: patients are sent to the dentist when the answer is actually in the sinus above it.
- Ethmoid sinuses — a honeycomb of small air cells sitting between your eyes. The ethmoid sinuses are the most anatomically complex and the most commonly involved in chronic sinusitis. They also share walls with the eye socket, which is why severe ethmoid infections can occasionally threaten vision.
- Sphenoid sinuses — the deepest sinus, positioned behind the nasal cavity near the base of the skull. When the sphenoid is inflamed, patients often describe a headache behind the eyes or at the top of the head — the kind that doesn't fit any standard headache pattern and is often misdiagnosed for years.
The Physics of a Blocked Chamber
The sinuses drain through openings that are, in engineering terms, remarkably small given the volume they serve. The maxillary sinus — roughly the size of a walnut — drains through an opening approximately 2–3 mm in diameter. The same Poiseuille's Law we covered in Issue 2 (nasal valve) and Issue 3 (turbinates) applies here: resistance to flow increases exponentially as the radius of the opening decreases.
When the mucosal lining swells even modestly — as it does in response to a cold, allergies, or environmental irritants — those already small openings narrow further. Drainage slows. The sinus lining continues to produce mucus, but that mucus has nowhere to go. Oxygen levels inside the sinus cavity drop. The environment shifts from aerated and self-clearing to stagnant and hospitable to bacterial growth.
This is not an infection that arrives from outside. In most cases of chronic sinusitis, it is an environment that the body itself creates — by failing to maintain the pressure and drainage that keep the plenum chamber functioning.
💡 THE OSTIOMEATAL COMPLEX — THE MASTER DRAIN
The ostiomeatal complex (OMC) is the shared drainage pathway where the frontal, maxillary, and anterior ethmoid sinuses all converge before emptying into the nasal cavity. Think of it as the main manifold junction of your plenum system. When the OMC narrows — from a deviated septum, swollen turbinate, or polyp — multiple sinuses can fail simultaneously from a single blockage point. This is why treating the OMC is the central goal of most modern sinus surgery.
🏎️ PADDOCK PASS — Behind the Scenes
“The Scope and the Map — Together”
I want to come back to Diana for a moment — specifically to what happened when I sat down with her and reviewed both her nasal endoscopy findings and her CT scan images together.
This is something I do deliberately with patients who have struggled to get answers: I pull the CT scan up on the screen alongside the scope images and walk through them in real time. The scope gives us the live view — what the lining looks like, where drainage is impaired, what the mucosal surface is doing right now. The CT gives us the map — the three-dimensional architecture of the sinuses, the bony framework, which cavities are involved, and exactly where the drainage pathways are narrowed or blocked.
Neither one tells the full story alone. The scope without the CT is like reading a weather report without a satellite image — you can see what’s happening at the surface, but you can’t see the system driving it. The CT without the scope is a map of a city you’ve never walked. Together, they give you the complete picture.
What Diana’s scope and CT showed together was this: her sinus drainage pathways were not blocked by polyps or a major structural defect. They were functionally obstructed — the mucosal lining around the ostiomeatal complex was chronically thickened and reactive, the drainage channels were swollen shut, and the sinuses had been running in a low-grade inflammatory cycle long enough that the system had essentially normalized that state.
“I kept thinking I was getting sinus infections,” she said, “because every time I saw a doctor, I got antibiotics.”
That’s the conversation that changed her care. Seeing both the scope and the CT together made it real — not a vague explanation of “inflammation,” but a visible, mappable system failure with a logical path forward.
For Diana, the path forward started with targeted high-volume nasal irrigation, a steroid spray regimen corrected for technique, and allergy evaluation — grounded in a clear understanding, from her own images, of why those interventions made sense for her specific anatomy. That kind of clarity is what three years of prescriptions hadn’t been able to give her.
Diagnosis: What We're Actually Looking For
Sinusitis is diagnosed clinically — based on symptoms, duration, and physical examination. But in chronic cases, the examination that matters most is the nasal endoscopy: a thin, flexible camera passed gently through the nose that gives a direct view of the middle meatus, the sinus drainage pathways, and the mucosal health of the nasal lining.
What I'm looking for: mucosal edema, purulence (active drainage from a sinus opening), polyps, and the status of the structures surrounding the ostiomeatal complex. A CT scan of the sinuses is the next step when medical therapy hasn't worked — it gives a roadmap of the anatomy and tells us exactly which sinuses are involved and where the obstruction lies.
HOW IS CHRONIC SINUSITIS DEFINED?
- Acute sinusitis: symptoms present for up to 4 weeks
- Recurrent acute sinusitis: 4 or more acute episodes per year
- Chronic sinusitis: symptoms persisting for 12 weeks or longer, despite treatment
Symptoms include nasal congestion, facial pressure or pain, cloudy nasal discharge, reduced sense of smell, and fatigue. The fatigue piece is consistently underappreciated — a chronically inflamed sinus system is an immune system under constant low-grade activation, and that carries a metabolic cost that patients feel every day.
Treatment: Opening the Manifold
Treatment follows the same engineering logic we apply across this series: identify the failure point, address the least invasive fix first, and escalate only when the system doesn't respond.
Step 1: Restore Drainage with Irrigation
High-volume saline irrigation is the single most evidence-supported intervention for chronic sinusitis. This is not a nasal spray — it is a flush: 100–240 mL of isotonic saline delivered with enough volume to wash debris, allergens, and inflammatory mediators from the nasal cavity and sinus drainage pathways. It works by reducing mucosal edema, improving mucociliary clearance, and physically removing the particulate burden that perpetuates inflammation.
Step 2: Reduce Mucosal Inflammation
Topical nasal steroid sprays — and in more severe cases, steroid-added irrigation (budesonide respules in the rinse) — target the mucosal swelling that narrows drainage pathways. Allergy evaluation and treatment is essential when allergic triggers are driving the inflammation. For patients with nasal polyps, biologic medications (dupilumab, mepolizumab) represent a major advance — they target the underlying inflammatory pathway rather than just suppressing symptoms.
Step 3: When the Hardware Needs Repair
When medical therapy cannot restore drainage — because the anatomy is too compromised, or polyps have filled the sinus cavities — surgery becomes necessary. There are two main approaches:
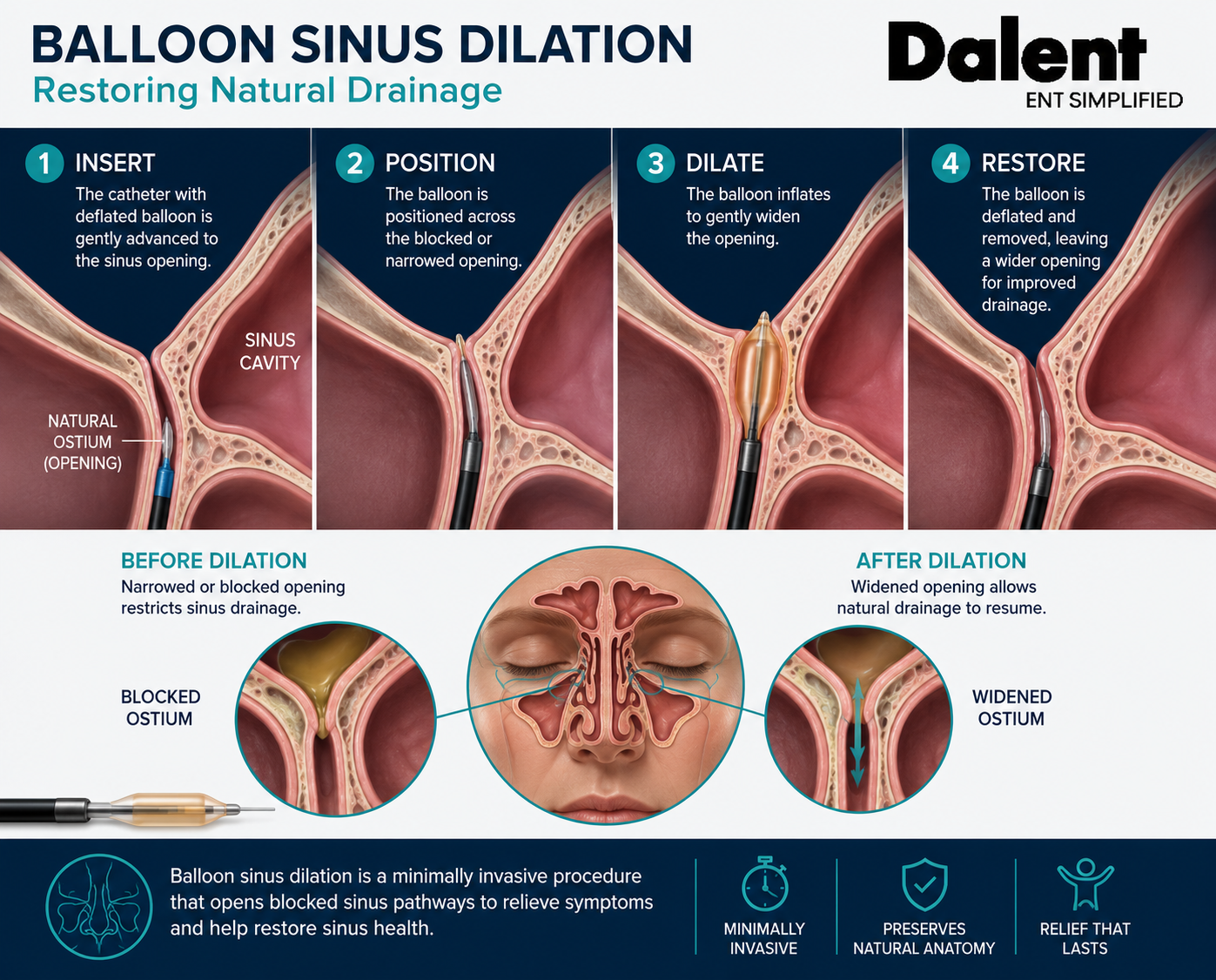
- Balloon sinus dilation — a minimally invasive office procedure in which a small balloon is advanced into the sinus ostium (opening) and inflated to widen it without removing tissue. Appropriate for patients with isolated, uncomplicated sinus obstruction and no polyps. Often combined with turbinate reduction.
🔬 PRODUCT HIGHLIGHT — DALENT MEDICAL
Full disclosure: I am a co-founder of Dalent Medical. So yes — this is a shameless plug. But I am including it here because it is a genuinely good example of the kind of engineering-forward thinking this newsletter is built around.
Dalent Medical is a medical device company built on one premise: that the structures of the upper airway deserve devices designed with the same precision and aerodynamic logic that engineers apply to high-performance systems. The same framework we use in this newsletter — airflow, pressure, resistance, drainage — is the engineering language behind Dalent’s device development.
Balloon sinus dilation is a perfect example of this philosophy in action. Rather than cutting or removing tissue to open a blocked sinus outflow tract, a precisely sized balloon is advanced into the narrowed opening and inflated to gently widen it — restoring drainage while preserving the natural anatomy. It’s the kind of intervention that treats the system as an engineered structure, not just a collection of parts to remove.
Most patients go home the same day. Many are back to normal activity within 24–48 hours. No general anesthesia required in most cases.
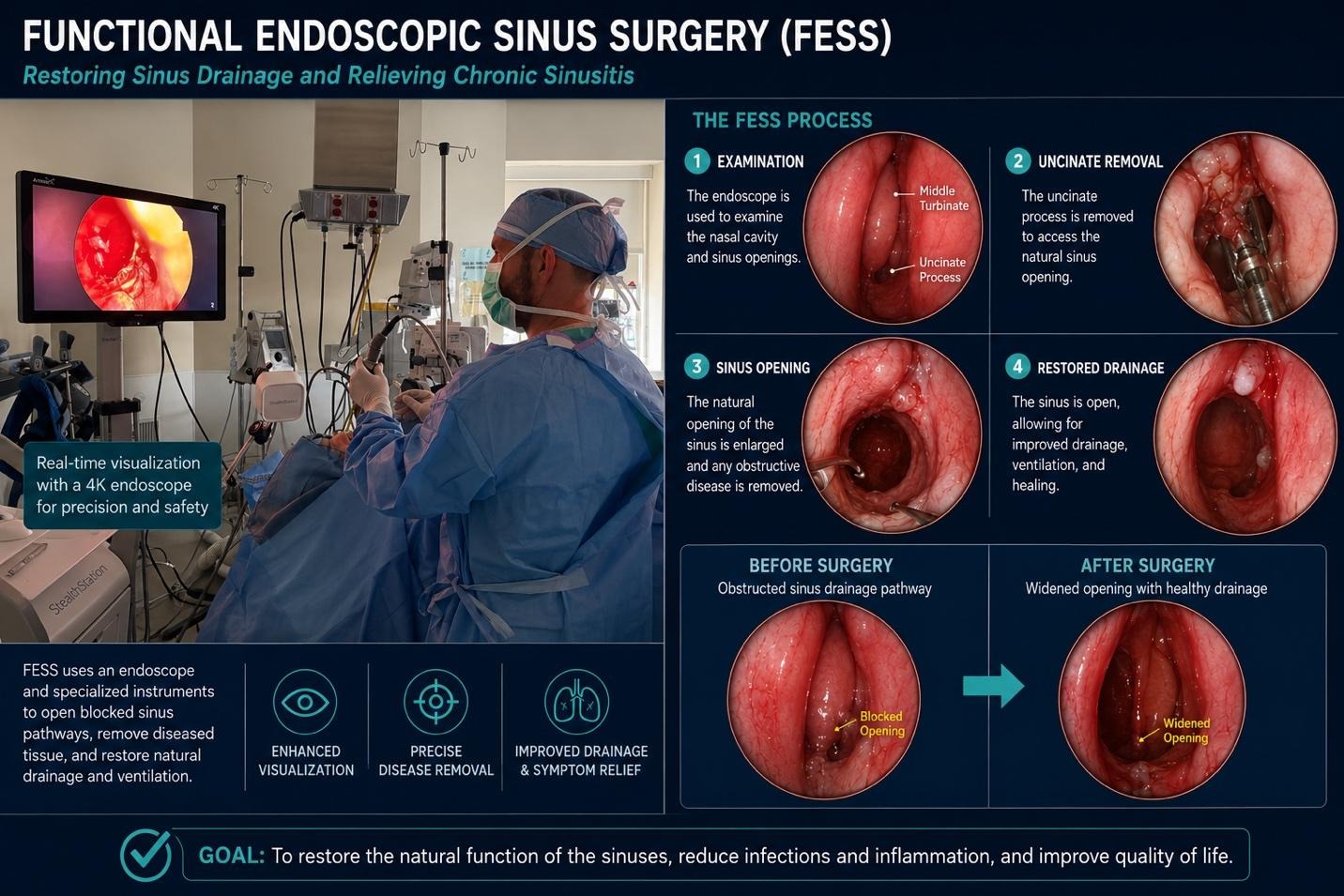
- Functional Endoscopic Sinus Surgery (FESS) — the standard surgical approach for chronic sinusitis that hasn't responded to medical therapy. Using a small endoscope and precision instruments, the surgeon removes tissue, polyps, or bone that is blocking the sinus drainage pathways. The goal is never to hollow out the sinuses — it's to restore the natural outflow tracts and allow the mucosa to recover.
⚡ DRS ENABLED — This Issue's Quick Win
⚡ DRS ENABLED — ONE ACTION YOU CAN TAKE TODAY
Upgrade your nasal rinse from spray to irrigation — and do it correctly.
If you're currently using a nasal spray for sinus symptoms, you're bringing a garden hose nozzle to a pipe-flushing job. Nasal sprays moisturize. Nasal irrigation flushes — and the difference in effect is significant.
Here's how to do it right:
- Use a squeeze bottle, neti pot, or pulsatile irrigator — volume matters. You want at least 100 mL per side, not a fine mist.
- Use isotonic saline — a pre-packaged saline packet dissolved in the correct volume of water. Not too salty, not plain water.
- This one is non-negotiable: use only distilled, sterile, or previously boiled water — never straight tap water. Tap water is safe to drink because your digestive system can handle the microorganisms in it. Your nasal passages cannot. There is a rare but documented risk of serious infection from an amoeba called Naegleria fowleri that can survive in municipal tap water. It cannot infect you through drinking — but it can through nasal irrigation. Distilled water from the grocery store costs less than a dollar. Use it every time.
- Lean over the sink, head tilted slightly, and let the solution flow gently — don't force it. Breathe through your mouth. The solution should come out the other nostril, not down your throat.
- Clean the device thoroughly after each use and air-dry it completely. A dirty rinse bottle is its own infection risk.
One rinse per day, done correctly, does more for your sinus health than most people achieve with an entire medicine cabinet of sprays. Start tonight.
📋 TECHNICAL REGULATIONS — This Issue's Safety Check
📋 KNOW WHEN TO STOP EXPECTING ANTIBIOTICS TO WORK
This is one of the most consequential misunderstandings I encounter in chronic sinusitis care.
Antibiotics are appropriate for acute bacterial sinusitis — when symptoms are severe, worsening after 10 days, or accompanied by high fever and significant facial pain. In that context, they are the right tool, and they work.
But chronic sinusitis is a more complicated picture. It is not simply a bacterial infection that persists because the antibiotic wasn’t strong enough. It is a condition in which bacterial colonization, mucosal inflammation, impaired drainage, and underlying contributors — allergies, anatomic narrowing, environmental triggers — all interact and reinforce each other. Antibiotics can address the bacterial component. They cannot reduce the mucosal inflammation. They cannot reopen a narrowed ostiomeatal complex. They cannot treat the allergic drive that keeps the lining reactive. And repeated courses, without addressing those other contributors, do not break the cycle — they just delay the next episode.
This is why patients with chronic sinusitis often describe years of antibiotic courses that work temporarily but don’t last. The infection clears. The underlying system dysfunction doesn’t. Three weeks later, the same environment that produced the last infection produces the next one.
The regulation:
If you have completed more than two courses of antibiotics for sinus symptoms in the past year without lasting improvement, it is time for a specialist evaluation — not another prescription. A nasal endoscopy, a CT scan, and a treatment plan built around the full picture — bacterial, inflammatory, anatomic, and allergic — is what the system needs. The rulebook is clear: the right tool for the right failure mode. And for chronic sinusitis, antibiotics alone are rarely the only tool the system needs.
CORE THESIS — ISSUE 5
Your sinuses are not hollow holes in your skull waiting to fill with infection. They are pressurized chambers in a precision-engineered drainage and ventilation system — one that, when functioning correctly, keeps your airway conditioned, your immune defenses active, and your breath flowing without effort.
When the plenum fails — when drainage narrows, pressure stagnates, and mucus can't clear — the entire downstream system pays the price. You feel it as facial pressure, blunted smell, persistent fatigue, and an immune system that can't stop fighting a battle it was never designed to sustain.
Restore the drainage. Reduce the inflammation. Fix the anatomy when needed. That's how you bring the plenum chamber back online.
The ENT Edge
Join Dr Gus on Substack for more actionable wellness insights and guides to help you sleep, breathe, and hear better, with spotlights on new technologies in the ear, nose and throat health category.

.jpg)